
Manual therapy management of elbow pain: a practicle clinical framework
Elbow pain is a common condition I see in both athletic and occupational patients, often persisting despite conventional rest and exercise advice. Traditional ‘epicondylitis’ models – lateral or medial – tend to over-emphasise tendon pathology while overlooking the myofascial, fascial and neural contributions.
In my clinical practice I see many variations of elbow pain and one of the very first objectives for me is to undertake the following assessment:
1. Establish the pathology.
2. Confirm if it is true elbow pain (local pathology).
3. Confirm if it is referred pain that mimics elbow pain.
4. Confirm if there is a neural component.
5. Confirm if this is overuse tendon pathology and what grade it is.
6. Confirm if it is an articular injury (joint, bone, cartilage).
7. Or, God forbid, all the above because those conditions do exist.
Elbow pain is frequently presented in manual therapy practice, whether from upper limb sports, repetitive lifting, computer use or occupational strain. While ‘tennis elbow’ (lateral epicondylalgia) and ‘golfer’s elbow’ (medial epicondylalgia) dominate clinical terminology, many persistent cases are multifactorial which can sometimes confuse the narrative of true elbow pain conditions.
It should be noted that hands on therapists often develop elbow pain conditions via overuse environments from overload to the forearm flexor/extensor muscle groups.
This article distils that approach into a cohesive clinical model suitable for practitioners seeking structured, evidence- informed guidance for elbow pain management.
Subjective assessment (history taking) is our first point of call and can rule out or in a lot of these considerations. For example, joint/bone/cartilage conditions will usually have a mechanism of injury attached to their history, such as trauma or an overuse of velocity forced upon the joint, such as the throwing athlete where there is a lot of load and tension thrust on the extension component of the elbow joint. The symptomology usually can be described as painful clicking, grinding and even locking of the joint. A lot of the time it is hard to palpate a hot spot or pain is diffuse. The pain can be described most as sharp and deep.
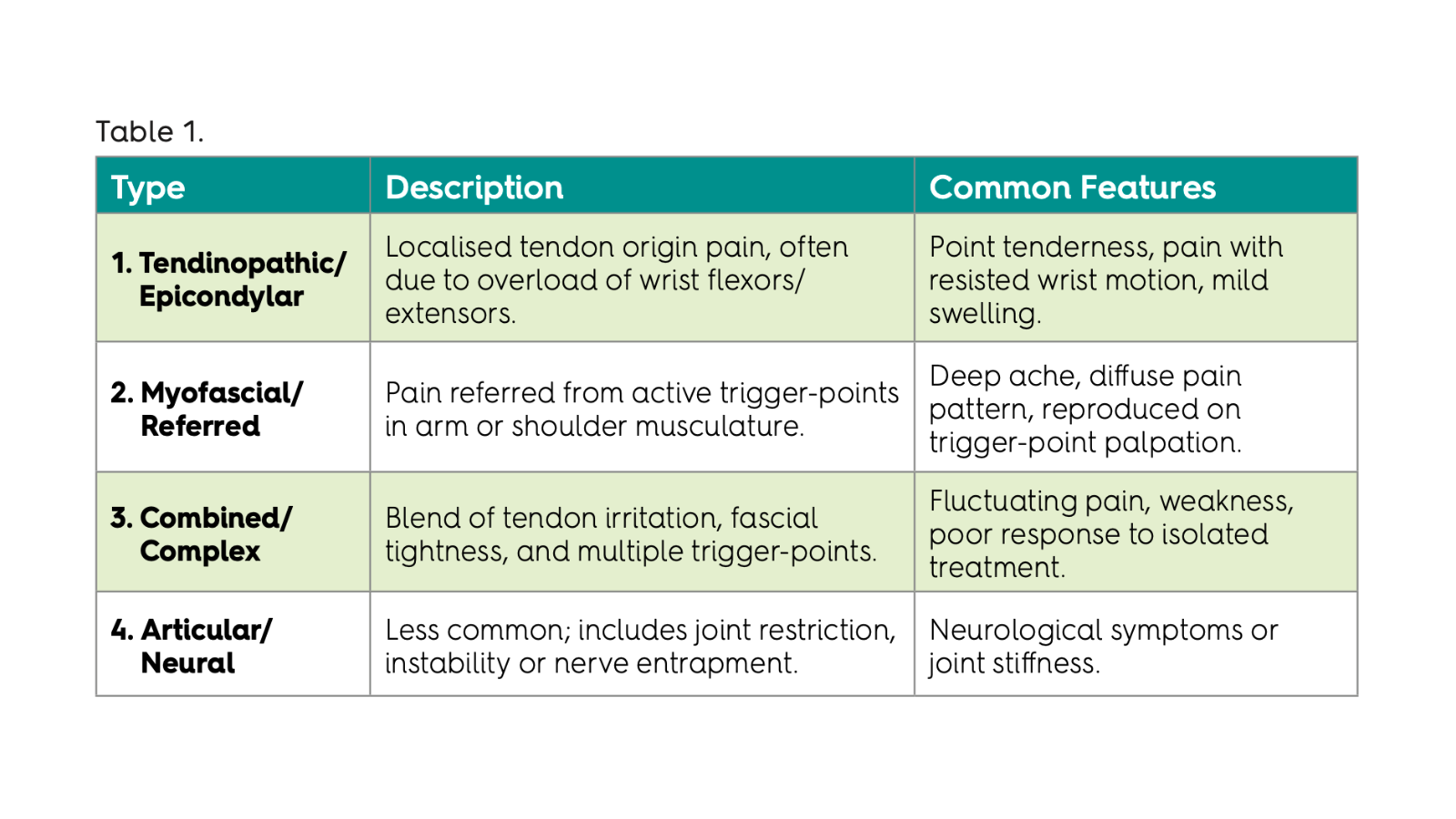
1. Classification of Elbow Pain
A clear classification supports targeted treatment. Elbow pain can be grouped into four broad categories (Table 1): This simple classification helps guide initial assessment and manual therapy focus.
2. Assessment Protocol
2.1 Patient History
Mechanism and duration of onset
Aggravating movements (gripping, lifting, computer work)
Previous injury or shoulder/neck pain
Occupational and training load.
2.2 Observation and Movement Testing
Observe posture and upper-limb alignment; assess range and quality of:
Elbow flexion/extension
Forearm pronation/supination
Wrist flexion/extension
Grip strength and endurance
Cervical quadrant test for facet joint
Compression test for disc or nerve root.
Palpate bony landmarks (epicondyles, radial head, olecranon) and note tenderness or tissue thickening. This is so important to rule in or out true elbow pathology such as tendon overuse conditions.
2.3 Soft-Tissue Palpation
This approach emphasises slow, precise palpation of each muscular compartment.
Key structures:
Be sure to rule out referred sites:
If you are not able to reproduce the patient’s symptoms, clinical reasoning should be looking for distal referral.
Local Palpation
Lateral side: ECRB, ECRL, ECU, supinator, brachioradialis, anconeus
Medial side: Pronator teres, FCR, FCU, palmaris longus
Posterior arm: Triceps brachii (all heads)
Elbow joint lines: Ligaments of the elbow joint.
Distal Palpation
Supraspinatus, infraspinatus, teres minor/major
Scalneus, 1st rib, pec minor
C4-7 facet joints.
Identify taut bands and reproduction of familiar pain – classic trigger-point signs.
2.4 Fascial Assessment
Test superficial and deep fascial glide. Gently move skin and subcutaneous tissues across compartments. Restrictions often occur at:
Inter-muscular septa between flexor and extensor compartments
Distal upper-arm fascia (linking biceps/triceps to forearm)
Lateral intermuscular septum connecting triceps to ECRB region.
2.5 Functional Testing
Ask the patient to perform grip, push, pull or lift tasks relevant to their daily demands. Observe compensations or asymmetry. This assists in linking soft-tissue findings to functional limitation.
2.6 Red Flag Screening
Always rule out cervical or neural pain (ulnar, radial, median nerve entrapments) and systemic causes (rheumatoid, gout, fracture) as these will be rare but more sinister symptoms such as extreme tenderness, feeling unwell and fever will exist. If in doubt, refer to a medical practitioner to diagnose.
Tendon Overuse Condition
We need to be vigilant when dealing with overuse tendon injuries and be sure to match the signs and symptoms to the stage and classification they present with.
Tendon Overuse
Tendon overuse injury can be more associated with doing a lot of repetitive actions on the tendons of the forearm flexors or extensors, especially something that you are not accustomed to doing, the tendon reaches a threshold of capacity and starts to affect the tendon structure dysfunctionally. For example, excessive gripping, such as digging holes in hard clay or hammering in nails in a deck. Positive assessment signs are easily reproduced by gripping or squeezing one’s hand as hard as possible, by resisted wrist extension, flexion, supination or pronation of the elbow, or by palpation of the attachment of the common flexor or extensor tendon to the bone, which will reproduce and highlight a hot spot. The symptoms can vary from slight discomfort to sharp pain. In these cases, weakness, such as holding a coffee mug or just going from a flexed elbow position to extension are clear markers.
1. Reactive Tendinopathy (Early/Acute Overuse)
What is happening in the tendon:
Tendon responds to overload with non-inflammatory thickening
Cells increase protein production to protect the tendon
No tendon tearing.
Clinical features
Pain during or shortly after activity
Pain settles quickly with rest
Minimal or no strength loss
Often recent increase in load (new sport, heavier work).
Examples
New tennis player
Sudden increase in gripping or repetitive manual work
KEY POINT:Reversible stage with appropriate treatment, tendon loading rehab and load management.
2. Tendon Disrepair (Subacute/Failed Healing)
What is happening in the tendon:
Disorganised collagen
Increased blood vessels and nerves
Early structural change.
Clinical features
Pain during activity and persists after
Morning stiffness around elbow
Reduced grip strength
Symptoms present for weeks to months.
Examples
Office or trade worker with persistent elbow pain
Pain with lifting, gripping or typing.
KEY POINT: Still treatable, but requires structured rehab, not just rest which usually prolongs the healing. Tendons need load to heal but the right amount, this is why supervised tendon loading rehab is so important.
3. Degenerative Tendinopathy (Chronic)
What is happening in the tendon:
Cell death and collagen breakdown
Weak areas within the tendon
Little to no inflammation
Clinical features
Pain may fluctuate or be constant
Marked weakness and functional limitation
Poor response to rest alone
Symptoms >3–6 months.
Examples
Long-standing tennis elbow that ‘never fully settles’
Pain even with light tasks.
KEY POINT: Structural changes are largely irreversible, but symptoms and function can improve with rehab. This is the nasty classification of tendon injuries, which in athletes can be career ending. Consultation with a sports and exercise doctor to overview all medical options is important. Soft tissue therapy can still be warranted, especially dry needling to reduce hypersensitivity. Hands-on techniques should be targeted to surrounding tissue to address secondary issues that arise.
4. Partial Tendon Tear (Advanced Stage)
What is happening in the tendon:
Localised tearing within the tendon
Often superimposed on degenerative tendon.
Clinical features
Sharp pain with loading
Sudden loss of strength
Pain localised to a small area
Imaging (US/MRI) may confirm tear.
KEY POINT: Higher risk of rupture; management must be cautious.
5. Tendon Rupture (Rare at Elbow)
What is happening:
Complete tendon failure.
Clinical features
Sudden severe pain
Functional loss
Often associated with trauma or corticosteroid injections.
KEY POINT: Surgical management is usually required.
Alternative Simple Clinical Grading (Pain-Based)
Some clinicians use a simpler grading system:
Grade 1 Pain after activity only
Grade 2 Pain during and after activity, no strength loss
Grade 3 Pain during activity with strength loss
Grade 4 Pain with daily activities and marked weakness.
Important Clinical Notes
‘Tendinitis’ is a misnomer – most chronic elbow tendon pain is degenerative, not inflammatory
Pain does not always correlate with imaging severity
Early identification improves outcomes significantly.
Soft tissue therapy is primarily best indicated in Grade 1/2 stages for early resolution, in conjunction with a supervised tendon loading rehab program. As far as Grade ¾ stages are concerned, yes we can still treat, but with the understanding that resolution is unlikely in a short period of time. As mentioned before, a sports physician should be consulted for all available medical options.
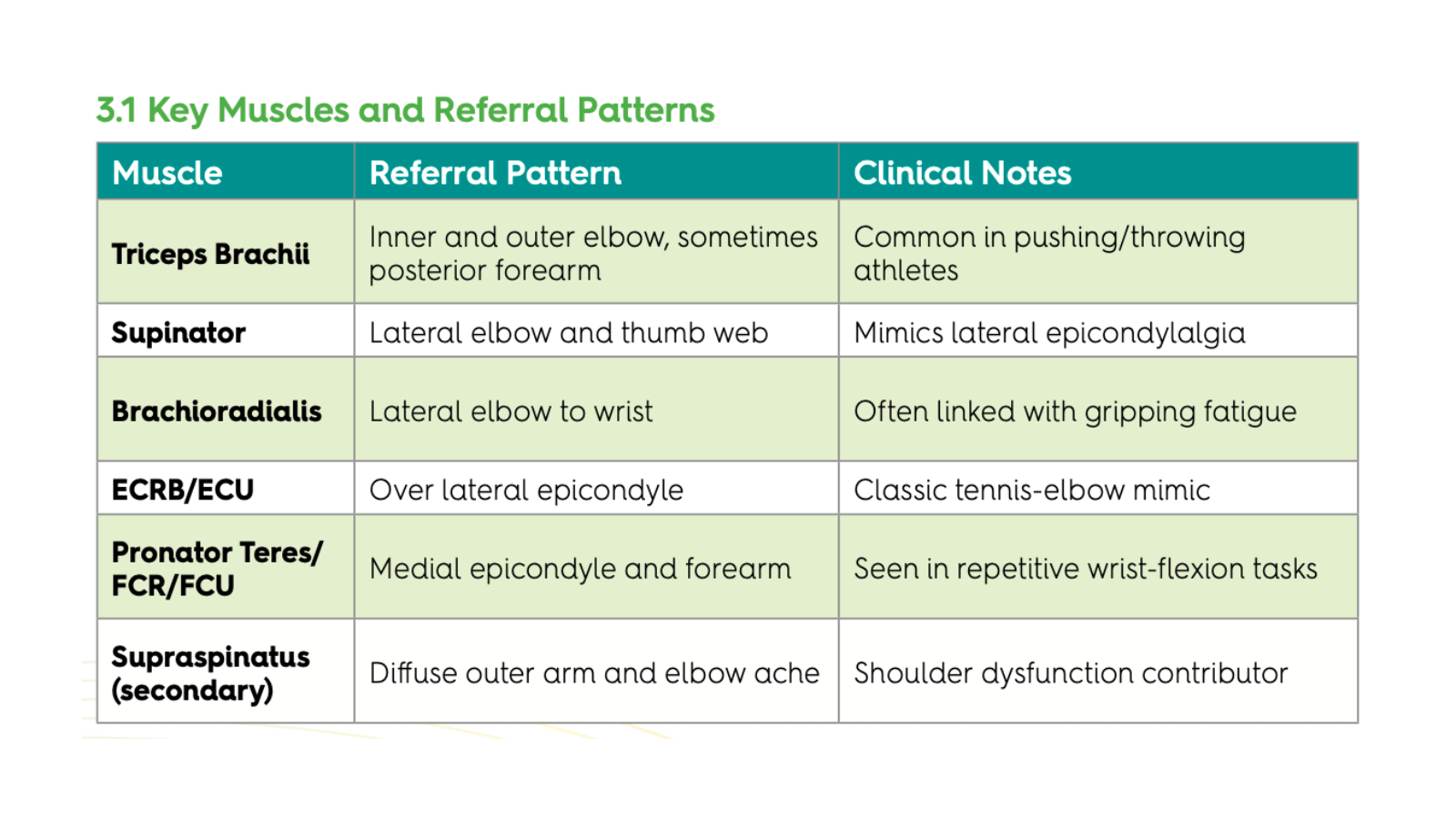
3. Trigger-Points Referring to the Elbow
Myofascial Trigger Points/Ligament
When we start talking about referred pain either from myofascial trigger points or neural conditions the overuse or trauma history may not exist as so obvious as in a tendon bias condition, so we are left wondering the ‘how, what and where’. From a trigger point view, the most likely candidates can come not necessarily from forearm flexors or extensors as they refer to the wrist/hand and distal forearm, we need to be mindful that their triceps/supraspinatus even the scalenes are more likely to refer to the elbow joint.
It is important to keep in mind that muscles, such as anconeus, can mimic elbow pain. It’s responsible for that lock outcomponent on extension of the elbow, so makes a prime target for elbow pain. I also take into consideration the ligaments of the elbow, such as medial/lateral collateral, radial collateral and even the annular ligaments which can house trigger points. Most of these ligaments will usually refer down the forearm and even to the wrist and hand, but this is where our palpation skills serve us best in isolating pain and symptom reproduction.
3.2 Treatment Strategies
Identify painful sites using grip strength.
Grade hypersensitivity with palpation, if highly irritable, dry needling to the trigger points or painful lesions.
Treat with deep sustained longitudinal strokes (always start distal to painful sites and continue past to proximal).
Treat, reassess and treat again until pain plateaus out using grip strength.
Follow up with passive release techniques to forearm extensors/flexors and triceps.
Post-release stretch and active movement.
Follow with gentle mobilisations of the elbow joint.
Deactivation often results in immediate pain reduction and increased grip strength.
4. Fascial Restrictions and Kinetic-Chain Influence
4.1 Fascial Connections
The elbow sits at the intersection of several myofascial continuities:
Superficial Back Line: links triceps to forearm extensors and dorsum of hand
Superficial Front Line: links biceps to forearm flexors and palm fascia
Lateral Line: connects deltoid–triceps fascia to radial wrist extensors.
Restriction along these chains – particularly near the intermuscular septa – can perpetuate loading imbalances.
4.2 Identifying Restrictions
Restricted fascia may feel ‘leathery’ or immobile beneath the skin. Hinds’ method includes:
Slow shearing movements perpendicular to fascial lines
Longitudinal glide following fascial chain to the shoulder.
4.3 Treatment Approach
Myofascial tension techniques, engage and place a shear tension to challenge tissue
Gentle stretch combined with breathing to release neural/fascial tension
For tendon overuse conditions myofascial dry needling can be indicated.
Fascial work is especially valuable in chronic, load-resistant cases of epicondylalgia.

5. Practical Manual Therapy Protocol
Session 1: Initial Assessment and Treatment
Goals: Reduce pain, identify key soft-tissue dysfunctions, introduce self-care.
1. Assess tissues with effleurage and longitudinal strokes – this helps us identify hidden areas of sensitivity and inconsistency in the tissue.
2. Target trigger-points to ECRB, ECU and triceps proximal trigger points.
3. Perform fascial release along forearm/tricep compartments.
4. Assess and treat neural restrictions (cervical, peripheral nerve entrapments ie: radial, ulnar, median nerves). The goal is to restore full neural mobility.
5. Myofascial dry needling to areas of hypersensitivity (best indicated when hands on tissue techniques are contraindicated).
6. Rocktaping/Kinesotaping post treatment to offload areas of hypertonicity and pain.
7. Educate patients on self-massage, neural mobility gliding and discuss acceptable load management.
Sessions 2–4: Restoration Phase
Goals: Improve tissue extensibility, restore load tolerance.
1. Re-assess tenderness and range.
2. Introduce deeper trigger-point release, fascial driven techniques, assess and treat neural considerations.
3. Begin eccentric loading for wrist extensors/flexors.
4. Reinforce shoulder and postural correction if applicable.
Sessions 5+: Integration & Prevention
Goals: Return to full function, prevent recurrence.
1. Educate on workplace or sport-specific ergonomics.
2. Prescribe ongoing self-trigger-point maintenance.
3. Schedule periodic soft tissue ‘tune-ups’.
6. Case Application Example
Patient: 42-year-old office worker, right- dominant.
Complaint: Chronic lateral elbow ache for six months.
Assessment: +ve grip test, resisted wrist extension, elbow supination.
Findings: Active trigger-points in ECRB, ECU and lateral triceps; fascial tightness along lateral line; normal joint motion, restricted radial nerve mobility (neurodynamic testing).
Treatment: Three sessions over two weeks of dry needling to proximal tendon, trigger-point release, fascial glide and radial nerve treatment (main site of restriction was supinator interface) followed by progressive eccentric loading.
Outcome: Pain reduced from 7/10 to 1/10; grip strength full; maintenance every four weeks for two months.

Self-Care and Patient Education Home program:
Daily self-trigger-point release (ball or fingers)
Forearm stretching (flexors and extensors) 3 x 30 seconds
Warm-up before repetitive activity
Postural awareness (shoulder retraction, neutral wrist)
Regular movement breaks in desk work
Education empowers patients and prolongs treatment outcomes.
Please look forward to part two of this article coming out shortly.