
Trigger Points ‘relief or resolution’
The purpose of this article is to promote discussion on the subject of treatment of trigger points based on clinical experience of massage therapists albeit any body worker. The views expressed in this article are purely mine with references to published peers. The article presents two views to widen our scope of treatment options, especially when dealing with the common bread and butter technique of trigger point therapy.
Over the years I have had the good fortune of being involved with lecturing in the practical aspects of massage/soft tissue therapy, more so at the remedial level, however I have also been involved with students in their first year of tuition. It is at this stage you are introducing the component of therapeutic massage techniques, which involves their first opportunity to apply techniques at a deeper level and to areas of tenderness. So the questions begin, why is it tender? How did it become tender, weak etc? And what techniques should we use to treat it or assist us in treatment?
I have had many lengthy discussions on the various theories associated with the effectiveness of treatment to trigger points and the development of trigger points, some from within the classroom, to corridors of clinic, uni, from the table of peers and all at various levels of interpretation and understanding. My discussion starts with the opinion that many therapists I have spoken with over the years hold and that is to treat TP`s effectively find the cause and treat. This is where opinions differ on the cause or causes. Some believe treating locally and aggressively provides resolution to the patient’s trigger point condition and others believe a broader approach is more effective. These two views form the discussion of this article. In discussion of the first point of view, I will look to the work of `Travell and Simons` authors of ‘Myofascial Pain and Dysfunction’ have written two extremely comprehensive references, an entire life’s work.
More information than one could ask for, from the body of work we can find comprehensive information on issues such as:
• What is a trigger point?
• The types of trigger points.
• How they develop?
• The common trigger point regions.
• Detailed muscular anatomy
• Muscle innervation, sensory levels and even biochemistry related to trigger points.
The latest edition includes a more tactile approach to treatment of trigger points but also includes reference to a research study that will form the first view. This study raises the question “Can repeated local treatment to TP sites induce long term resolution to the trigger point condition?”
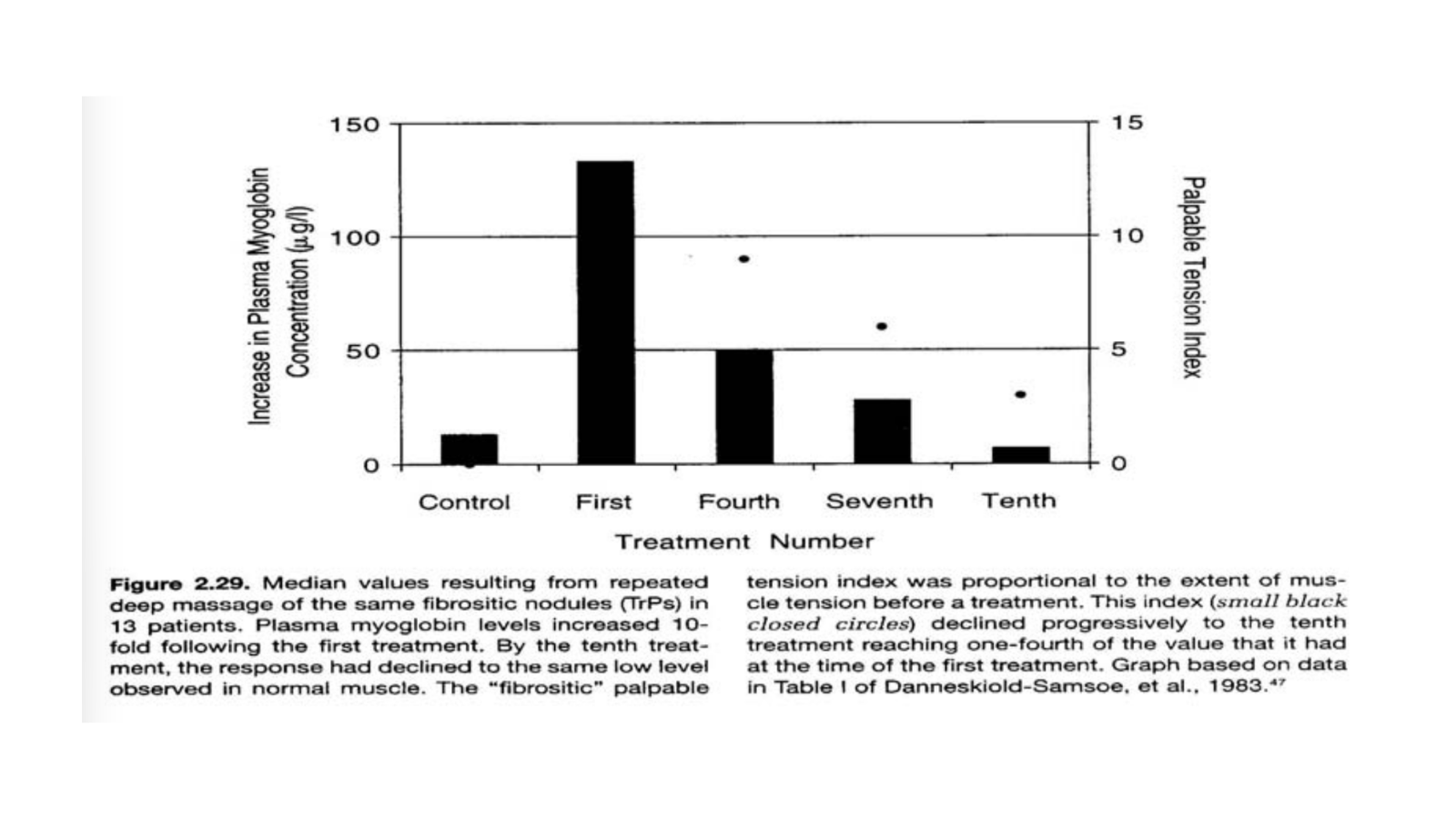
This view is supported by Danneskiold- Samsoe B, Christiansen E, Andersen in 1986 stated ”the myoglobin response to massage of fibrositic nodules can be explained on the basis of the observed histopathological changes in nodules. Repeated deep massage of the fibrositic nodules (TrPs) produced transient episodes of myoglobinuria that were not produced by similar massage of normal muscle the intensity of myoglobin response, the degree of tenderness, and firmness of the nodule progressively faded out with repeated treatments. If massage applied by the therapist resulted in cell rupture, the cell would spill myoglobin and most likely destroy the involved neuromuscular junction as a functional structure, thus effectively terminating the contracture and associated energy crisis. As more and more contraction knots within the nodule were eliminated, the patient would experience increasing relief of symptoms (1)”. See Graph*.
This study presents an interesting insight to the clinical experience to treating trigger points. Very rarely have I treated a trigger point and accomplished a complete resolution of tenderness, contracture of the taut bands within the one or two treatment sessions. I think we should keep in mind that by the time a trigger point has become active it has reached certain thresholds to get to that state, which would have taken some time. So maybe repeated treatments of the area over a period of time is logical.
I would like to discuss the second view of this article it will be highlighted using the research article on lower back pain `soft tissue or bone problems ` by Karen Morrissey` from last years A.M.T.A. journal Vol. 12 No.3 .It trialled 4 different soft tissue treatment scenario’s to lower back pain on four different subjects, treatments were once a week for five weeks. One of the treatment scenarios was using a trigger point protocol. The articles discussion of the treatment outcomes produced a familiar out come with treatment effective in reducing pain. By the end of the trial the patient had experienced five days pain free however re injured them, no long-term resolution. Is it then likely that if this patient had not re injured themselves then a possibility of resolution to their ongoing back pain could have been achieved, or was the cause of the re injury part of an underlying problem? The article went on to include other protocols, regarding treatment to structure and function and finally a combination of all three protocols to the region. The summary concluded that the approach that involved the combination of techniques reported the most benefit.
To further support the broader view, Lee and Vleming stated in1997 on treatment of pelvic instability the following case scenario of common hamstring and sacroiliac joint dysfunction, “Clinically the gluteus maximus appears to become inhibited whenever the SIJ is irritated or in dysfunction. The consequences to gait can be catastrophic when the gluteus maximus is weak. The stride length shortens and the hamstrings are overused to compensate for the loss of hip extensor power. The hamstrings are not ideally situated to provide a force –closure mechanism, and in time, the SIJ can become hypermobile. This is often seen in athletes with repetitive hamstring strains. The hamstrings remain overused and vulnerable to intramuscular tears (2)”.
It is my view that this case scenario will more than likely present with a trigger point component i.e.: gluteus medius, piriformis, obturator internus, sacrotuberous ligament and the hamstring proximal to distal regions depending on the athlete, plus or minus the referral patterns. If we were to treat the above TP condition locally with Danneskiold-Samsoe B, ChristiansenE, and Andersen 1986 study in mind what would our treatment goals offer relief or resolution?
My clinical experience in treating trigger points has lead me to not only assess the region of tenderness but also the muscle it is housed in:
• the structure it attaches to
• the function of that structure
• the antagonists and their structure and function,
• The referral sites also their structure and function.
• Are the tissues in a weak and lengthen state,
• Or the opposing state of adaptive shortening?
I believe that these questions play an important role in providing a more detailed picture of the dysfunction. The broader picture it presents is the question I feel we need to be answering when trying to achieve long-term resolution to the trigger point treatment.
I also believe that isolated treatment of these points of myofascial distress as the main concern in this dysfunctional picture can be compared to the view to switch off fire alarm without locating the source of the fire is probably short sighted. Should we then look further to the body’s structure? Presented will be possible structural imbalances to the pelvis, lumbar and thoracic spine and the functional condition. Soft tissue structures such as the quadratus lumborum in a shorten state on symptomatic side, lower portion of psoas at the femoral attachment, iliacus, Tfl, rectus femoris. Determining hip restrictions compare internal/external rotation, flexion/extension, and abduction/adduction. Compare slump test, treat to make even.
Some practioners who treat structural causes will find them and treat them, and others who look for functional causes will also do the same. Also a practioner with the understanding that bones being out of place will lead to adjustments and manipulations to restore normality. All of these approaches have benefit however; the approaches individually do not address the somatic dysfunction.
Chaitow in 2001 explains in his foreword remarks to Myers ‘Anatomy Trains’ book “The broader the view, the more likely it is the causes will be identify and dealt with (signs andsymptoms), in contrast attention being focused on regional areas and symptoms. Identification of shortness, weakness, tightness, restriction etc does not isolate a cause, but rather notes an effect, often result of distant influences. Function and structure can’t be separated any more than the mind from the body” (3).
I conclude that from a teaching point of view using one or two particular references to teach from, (such as book or from the charts) may support only one off these treatment types and present a limited scope towards our treatment. Although the questions from the first and second year students can become a task to answer, the solution maybe to introduce parameters, for use in a clinical picture until such time that the student can start to view the importance of the relationship between structure and function when treating somatic dysfunction as well as understanding that treatment of trigger points plays an important part but a small part in a larger picture.
POINTS TO REMEMBER:
“Trigger points are the physical manifestations of other problems.”
• Treating the cause will usually enable eradication of the point.
• Treating the point will relieve the symptoms.
• Treating the symptoms may or may not have any effect
The question I have addressed in this article is “Should we treat the subject of the development and treatment of trigger points with a broader view in mind, maybe as symptoms of a bigger picture?” The conclusion is “I believe so”, otherwise we may remain forever restricted or isolated in our treatment views. The differences can be between giving relief or resolution.
REFERENCES
Chaitow, L: In MyersT; Anatomy trains. Churchill Livingstone: New York: 2001
Danneskiold-Samsoe B, Christian E, Anderson RB: Myofascial pain and the role Myoglobin. Scand J Rheumatology 15: 174-178, 1986 IN: Travell & Simons 1999, Myofascial Pain and Dysfunction, Volume 1, Second edition Pg 77 (Graph)
Lee, D.Treatment of pelvic instability. In: Vleming A, Mooney V, DormanT, Snijders C, StoeckartR, eds.Movement, stability and low back pain. Edinburgh: Churchill
Danneskiold-Samsoe B, Christiansen E, Andersen RB: Myofascial pain and the role of myoglobin. Scand. J Rheumatology 15: 174-178, 1986